Type 1 diabetes: How to tackle the disease in children
Type 1 diabetes is a chronic condition that usually appears in adolescence when the pancreas makes little or no insulin.
Table of contents
Introduction
Type 1 diabetes is a chronic condition where the pancreas's beta cells or insulin-making cells make little or no insulin. This chronic insulin-dependent diabetes was once known as juvenile diabetes, as it was seen more in children and young people, but type 1 diabetes can develop at any age. Type 1 diabetes has no cure; the treatment focuses on managing blood sugar levels using insulin, diet, and lifestyle to prevent other complications.
What causes type 1 diabetes?
The exact cause of type 1 diabetes is unknown. The possible causes include:
Autoimmunity
It is a condition where the body’s immune system mistakenly destroys the healthy cells and organs of the body. Type 1 diabetes is thought to be mainly due to autoimmunity, where the immune system attacks the beta cells of the pancreas, thus affecting insulin production.
Genetics
It is another factor that leads to type 1 diabetes. Certain genes passed from parents to the child could cause type 1 diabetes.
Viruses
Exposure to viruses and other environmental factors could lead to type-1 diabetes.
The role of insulin in type 1 diabetes
The body uses glucose as the primary source of energy. The glucose enters the bloodstream by breaking down the carbohydrates from the diet. The beta cells produce insulin, which lets glucose enter the body's cells to provide energy. Any damage to the beta cells would affect insulin production, and the glucose does not move into the cells resulting in high blood glucose levels.
Symptoms of type 1 diabetes
Symptoms of type 1 diabetes include:
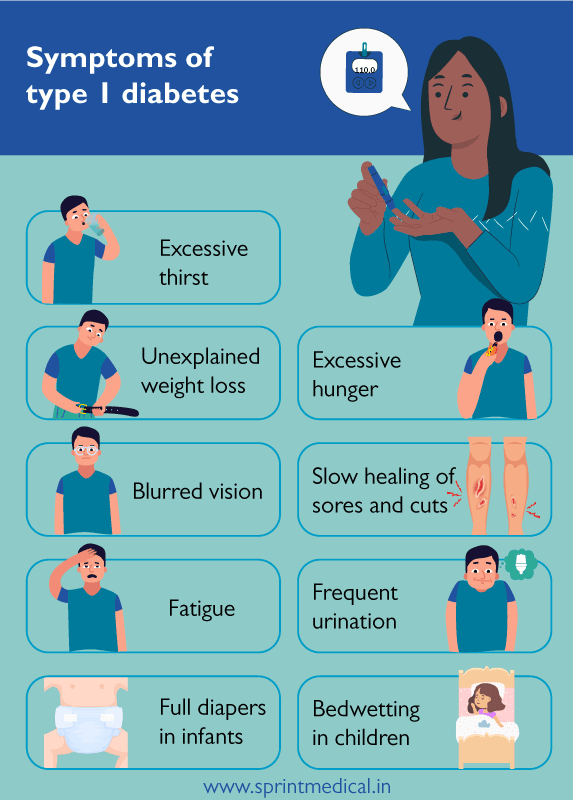
Excessive thirst
Unexplained weight loss
Excessive hunger
Blurred vision
Slow healing of sores and cuts
Fatigue
Frequent urination
Full diapers in infants
Bedwetting in children
Complications of type 1 diabetes
Type 1 diabetes could affect the human body's major organs over time. High blood glucose levels lead to various complications involving the heart, kidneys, eyes, blood vessels, and nerves.

Blood vessel and heart diseases
The complications involving the blood vessels and heart include coronary artery disease with angina (chest pain), heart attack, stroke, atherosclerosis (narrowing of the arteries), and high blood pressure.
Nephropathy or kidney damage
High glucose levels in the blood could damage the kidneys over time and lead to end-stage kidney diseases. The treatment options for end-stage kidney diseases are dialysis and kidney transplant.
Eye damage
Diabetes can cause serious eye damage like diabetic retinopathy leading to blindness, cataract, and glaucoma.
Neuropathy or nerve damage
Injury to the walls of the capillaries (tiny blood vessels) that feed the nerves causes numbness, tingling, and pain or burning sensation. These sensations commonly begin at the tip of fingers and toes and move upwards. Failure to manage high blood glucose levels over some time could cause the loss of all sensations in the affected limb.
Mouth and skin diseases
Uncontrolled diabetes increases the risk of fungal and bacterial infections in the skin and mouth. Rashes, blisters, dry mouth, and gum diseases are common in patients.
Diagnostic tests for type 1 diabetes
Type 1 diabetes can be diagnosed easily through blood and urine tests.
A blood test showing high blood glucose levels and the presence of autoantibodies indicates type 1 diabetes.
Urine test for ketones:
The human body generally uses glucose as a source of energy. In type 1 diabetic patients, the glucose does not move into the cells, making the body use the stored fats as an energy source. Burning fats for energy produces ketones; their presence in the urine indicates type 1 diabetes.
Management of type 1 diabetes in children
Type 1 diabetes has no cure; thus, the treatment focuses on managing blood sugar levels using insulin, diet, and physical activities.
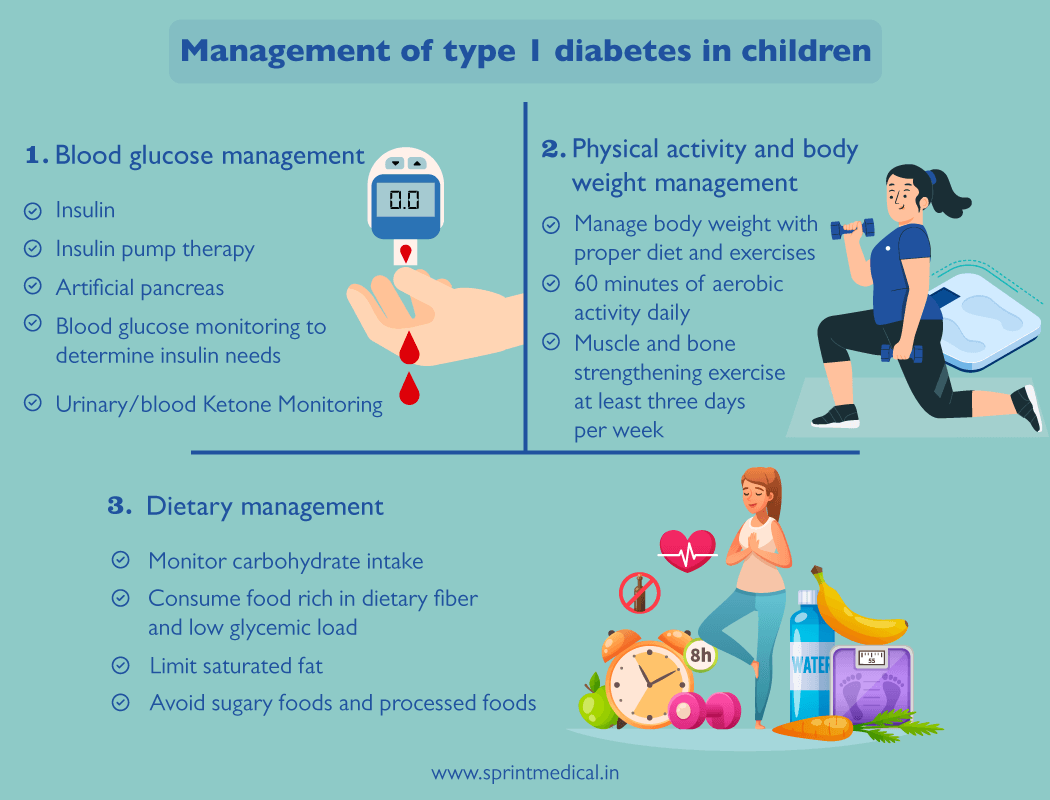
1. Blood glucose management
a. Insulin
Insulin therapy is critical for survival in all people with type 1 diabetes. Intensive insulin regimens can prevent the risk of developing complications in teenagers through multiple daily injections of prandial and basal insulin. The insulin regimen helps to mimic the regular insulin secretion patterns and achieve near-normal glycemic control.
Insulin doses for children on multiple daily injections (MDI) routine:
The initial daily insulin dose is calculated based on the patient’s weight. A child newly diagnosed with type 1 diabetes initially requires a dose of about 0.5 - 1.0 units/kg. One unit of insulin will process anywhere from 12 - 15 grams of carbohydrates and lower blood sugar by nearly 50 mg/dL.
The MDI (multiple daily injections) routine includes delivering long-acting insulin once a day in the morning or evening (sometimes twice a day in about 20% of patients) and rapid-acting insulin before snacks or meals. The long-acting insulin takes several hours to work and lasts about 24 hours, and rapid-acting insulin starts to work in about 15 minutes and continues to work for 2 - 4 hours. The doses are adjusted based on the carbohydrate intake and blood glucose level to achieve the blood sugar target.
b. Insulin pump therapy or continuous subcutaneous insulin infusion
Insulin pumps are an alternate setup for insulin delivery in children with type 1 diabetes. Recent studies show that children treated with insulin pumps have lower A1C (HbA1c - glycated hemoglobin) levels, improved diabetes-related quality of life, less fear of hypoglycemia (a condition where the blood glucose level falls below the standard range), and higher treatment satisfaction. Incorporating CGM (continuous glucose monitor) device with the insulin pump demonstrates notable improvement in both hypoglycemia reduction and glycemic control in children.
A1C should be measured at 3-month intervals in all adolescents and children with type 1 diabetes to assess their overall glycemic control.
c. Artificial pancreas
Artificial pancreas or closed-loop systems focus on enhancing glycemic control in type 1 diabetes. It includes a CGM in constant communication with an insulin infusion pump and a blood glucose device used for CGM calibration. An external processor like a smartphone receives the data from CGM and runs the control algorithm software. The amount of carbohydrates consumed is entered manually into the external device. The insulin infusion pump receives dosing instructions from the external device based on the carbohydrate input and CGM data.
d. Blood glucose monitoring to determine insulin needs
All adolescents and children with type 1 diabetes might need to have blood glucose levels monitored multiple times daily, including premeal and pre-bedtime, and as required for safety in specific situations such as driving, exercise, and the presence of symptoms of hypoglycemia or illness.
SMBG (Self-monitoring of blood glucose) levels is essential in treating type 1 diabetes in children. Routine SMBG determines immediate insulin needs (e.g., mealtime), safety assessment (e.g., corrective action for or prevention of hyper- or hypoglycemia), and longer-term adjustment in insulin dosing regimens based on blood glucose patterns and trends.
Blood glucose targets vary with the patient’s age, insulin regimen, supervision levels, and other lifestyle issues to achieve as many glucose values as close to the target as possible without excessive hypoglycemia.
e. Urinary/blood Ketone Monitoring
The ketone levels need to be monitored in children with type 1 diabetes in prolonged or severe hyperglycemia and acute illness to determine if adjustment to treatment or referral to urgent care is required.
2. Lifestyle changes for children with type 1 diabetes
The lifestyle changes to help children manage diabetes focuses on dietary changes, regular physical activity, and weight management.
a. Dietary management
Dietary management or nutritional therapy is an essential element of the overall treatment plan, and it considers family habits, food preferences, cultural or religious needs, schedules, and physical activity. The key to achieving optimal glycemic control is monitoring carbohydrate intake.
Carbohydrate intake from fruits, vegetables, legumes, whole grains, and dairy products, with a focus on foods higher in fiber and lower in glycemic load, is preferred over other sources containing added sugars. Saturated fats should be limited. Caloric intake should fuel normal growth and development and avoid being underweight and overweight.
3. Exercise and weight management
Exercise is advised for all youth with type 1 diabetes with the goal of 60 min of moderate- to vigorous-intensity aerobic activity daily and vigorous muscle-strengthening and bone-strengthening activities at least three days per week. However, education about preventing and managing potential hypoglycemia during and after exercise is crucial.
Periodic glucose monitoring before, during, and after exercise, with or without CGM use, is essential as it helps to prevent, detect, and treat hypoglycemia and hyperglycemia.
Approaches to prevent hypoglycemia during, after, and following exercise include reducing prandial insulin dosing for the meal preceding exercise, increasing carbohydrate intake, eating bedtime snacks, using CGM, and reducing basal insulin doses.
Given the present trends, at least one-third of adolescent patients with type 1 diabetes are obese or overweight. Proper and suitable diet and physical activity routines help to manage body weight.
1. Blood glucose management
a. Insulin
Intensive insulin regimen using prandial and basal insulin
Insulin pump
Artificial pancreas
b. Blood glucose monitoring to determine insulin needs
2. Lifestyle changes for children with type 1 diabetes
a. Dietary management
Monitor carbohydrate intake
Consume food rich in dietary fiber and low glycemic load
Limit saturated fat
Avoid sugary foods and processed foods
b. Physical activity and body weight management
Manage body weight with proper diet and exercises
60 minutes of aerobic activity daily
Muscle and bone strengthening exercise at least three days per week
Take-Home points
Type 1 diabetes is a chronic condition where the pancreas's beta cells or insulin-making cells make little or no insulin. Insulin lets glucose enter the body's cells to provide energy. Any damage to the beta cells would affect insulin production, and the glucose does not move into the cells resulting in high blood glucose levels.
This chronic insulin-dependent diabetes appeared mainly in children and young people and thus was known as juvenile diabetes, but type 1 diabetes can develop at any age.
The exact cause of type 1 diabetes is unknown. However, it is thought to be mainly due to autoimmunity, where the immune system attacks the beta cells of the pancreas, thus affecting insulin production. Other possible causes include genetics, viruses, and other environmental factors.
Type 1 diabetes has no cure; thus, the treatment aims to manage blood sugar levels using insulin, diet, and physical activities.
References
FAQs on Type 1 diabetes: How to tackle the disease in children
Type 1 diabetes is a chronic condition where the pancreas's beta cells or insulin-making cells make little or no insulin. As a result, the glucose does not move into the cells resulting in high blood glucose levels.
The beta cells in the pancreas produce insulin, letting glucose enter the body's cells to provide energy. When the beta cells make little or no insulin, the glucose does not move into the cells resulting in high blood glucose levels.
The pancreas produces insulin in type 2 diabetes but cannot use it effectively, or the body shows insulin resistance. But in type 1 diabetes, the beta cells produce little or no insulin. Moreover, lifestyle habits and diet do not cause type 1 diabetes and are less common than type 2 diabetes.
Type 1 diabetes could affect the human body's major organs over time. High blood glucose levels lead to various life-threatening complications involving the heart, kidneys, eyes, blood vessels, and nerves.
Patients with type 1 diabetes have higher blood glucose levels. The condition has no cure; thus, the treatment focuses on managing blood sugar levels using insulin, diet, and lifestyle to prevent other life-threatening complications.
Comments ( 0 )
No Comments
Leave a Comment
Related Posts
Berries and Diabetes: List of Berries for Diabetics to Eat
Berries don't cause as much of a spike in blood sugar as other fruits. These berries are also rich in fibre. We will learn more about berries and diabetes in this article.


Sayandeep
Can dehydration cause high blood sugar?
Diabetes mellitus is difficult to handle alone and when severe dehydration adds to it, it causes many complications and disorders like kidney disease

Manasa Krishna Perumalla
Health & Wellness Tips
Subscribe to our blog