20/01/2024 / Health and Fitness
Diabetes and Digestion: How does Diabetes affect your Digestion?
Learn how diabetes, both type 1 and type 2, can impact the digestive system, from gastroparesis and esophageal dysmotility to small intestinal and colorectal dysfunctions.
Table of Content
Introduction
Diabetes is a major global health problem that affects millions of people all around the world. Diabetes is characterized by persistent hyperglycemia and is caused by the body's inability to make or efficiently use insulin, the hormone responsible for regulating blood glucose levels. While the influence of diabetes on blood sugar regulation is well known, this complicated metabolic condition can also significantly impact other physiological processes of the body, such as digestion.
The digestive system is a remarkable and intricate network and plays a pivotal role in breaking down food, absorbing nutrients, and eliminating waste from the body. For people suffering with diabetes, however, this essential process is not immune to the repercussions of their condition. Elevated blood glucose levels can unleash a cascade of complications that interfere with the smooth functioning of the digestive system, potentially leading to a range of digestive disorders.
In this article, we dive deeper into the intricate relationship between diabetes and digestion. We will explore the mechanisms through which diabetes impacts different components of the digestive system.
What is Diabetes?
Diabetes is a chronic metabolic condition characterized by high blood glucose levels (sugar). The condition occurs when the body either doesn't produce enough insulin or cannot adequately use the insulin that it does produce. Insulin is a pancreatic hormone that regulates the intake and utilization of glucose by cells, giving energy.
Diabetes is classified mainly into two types - Type I diabetes mellitus and Type II diabetes mellitus. Both kinds of diabetes can result in hyperglycemia, or persistently high blood glucose levels. Chronic hyperglycemia can damage blood vessels and nerves over time, resulting in a number of complications affecting the eyes, kidneys, nerves, heart, and blood vessels. Diabetes increases the risk of cardiovascular illness, renal failure, nerve damage (neuropathy), and visual issues, among other things.
Link between diabetes and digestion
Diabetes affects almost every organ system in the body, and the severity and duration of the disease may have a direct impact on organ involvement. Though gastrointestinal (GI) issues are widespread in people with long-term diabetes, there is a lack of awareness about them.
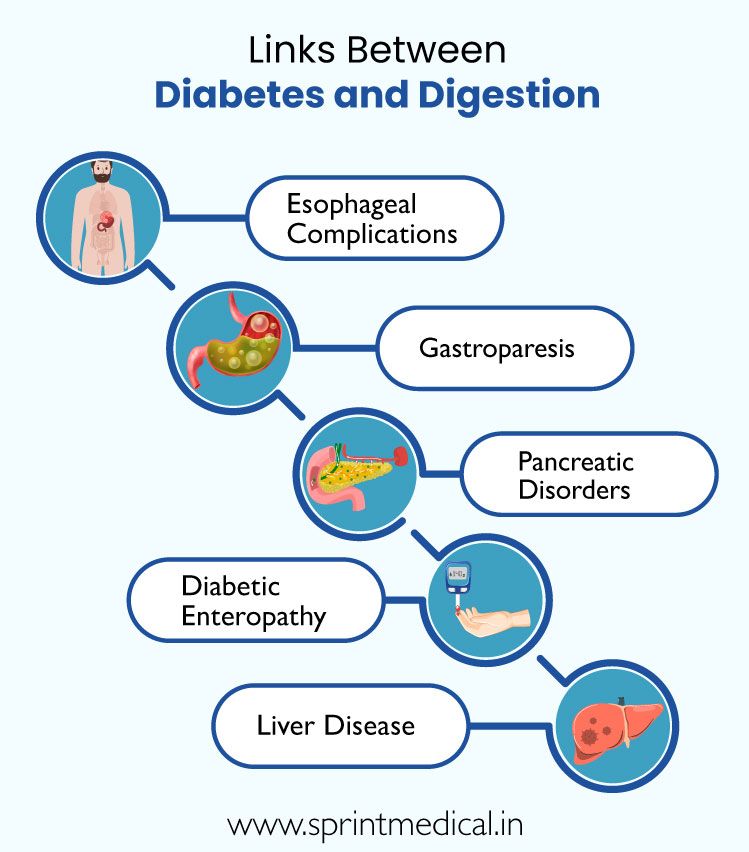
Diabetes and digestion have a complicated and multifaceted interaction since diabetes can impact numerous components of the digestive tract. The digestive process involves breaking down food into absorbable nutrients, which the body uses for energy and other vital tasks. Let's look at the fundamental links between diabetes and digestion:
Esophageal complications
Gastroparesis
Pancreatic disorders
Diabetic enteropathy
Liver disease
Esophageal complications
In humans, the thoracic esophagus and lower esophageal sphincter (LES) are composed of smooth muscle fibers innervated by the myenteric plexus. In Diabetic neuropathy, which is a complication of diabetes, particularly in those with longstanding diabetes, these autonomic nerves are affected. This impact manifests as neuropathy and structural remodeling of the esophageal musculature, resulting in anomalies such as abnormal peristalsis, spontaneous contractions, and reduced LES tone.
The prevalence of esophageal dysmotility in diabetes is reported to be as high as 63%. Notably, this dysmotility shows no significant difference between patients with type 1 and type 2 diabetes or between genders. Intriguingly, despite the high prevalence of esophageal dysmotility among patients with diabetes, only a minority experience classical symptoms such as dysphagia and heartburn. Gastroesophageal reflux symptoms are also prevalent in diabetes, reaching up to 41%.
Furthermore, there is an inverse relationship between glycemic control and gastroesophageal reflux disease. Improved glycemic control may contribute to better esophageal dysmotility and reflux outcomes. Along with medications to control these complications, patients are also advised to drink fluids immediately after taking medications to avoid the risk of pill-induced esophagitis.
Gastroparesis
Gastroparesis, one of the commonest gastrointestinal complications of diabetes mellitus. Gastroparesis is a digestive condition in which food remains in the stomach for too long (delayed gastric emptying), rather than passing into the small intestine when it should. Many individuals with type 1 and type 2 diabetes have evidence of delayed stomach emptying, with women more likely to have this condition. A substantial independent predictor of gastroparesis symptoms in people with type 2 diabetes and neuropathy has been discovered as obesity.
The cause of diabetic gastroparesis is multifactorial, involving factors such as elevated glycated hemoglobin levels, diabetes for more than 10 years, and the presence of other diabetes complications. Clinical signs and symptoms include vomiting, bloating, upper abdominal pain, early satiety, postprandial fullness, and weight fluctuations. Improved glycemic management or unexplained glycemic episodes should trigger a gastroparesis examination. Clinical manifestations might be acute, subtle, or chronic with frequent exacerbations. One third of patients have chronic symptoms.
General approaches to management of gastroparesis include ensuring good hydration, correcting electrolyte imbalances, management of diabetes and symptom reduction with medication.
Pancreatic disorders
The pancreas, an essential organ for controlling blood sugar levels, is significantly impacted by diabetes. When a person has type 1 diabetes, an autoimmune process occurs in which the body's defenses wrongly target and kill the beta cells that make insulin in the pancreas. As a result, the hormone insulin, which facilitates glucose uptake into cells, is either severely deficient or completely absent.
Type 2 diabetes, on the other hand, shows itself as insulin resistance, when cells stop responding as well to the effects of insulin. In order to make up for this, the pancreas initially produces more insulin, but over time, this might result in beta cell depletion and decreased insulin production. The pancreas becomes inflamed as a result of the chronically elevated blood sugar levels linked to diabetes, which may compromise the organ's structural stability and functional ability.
Long-term side effects could result in pancreatic fibrosis, a higher chance of pancreatitis, and, in certain situations, a higher risk of pancreatic cancer. The key to minimizing these diabetic complications is maintaining pancreatic function through adequate blood sugar control.
Diabetic Enteropathy
In individuals with longstanding diabetes, especially those with gastroparesis, small intestinal and colorectal dysfunctions are common, often presenting as diarrhea, constipation, or fecal incontinence. This occurs due to neuropathy of the nervous system of the gut and is known as diabetic enteropathy.
Diabetic enteropathy symptoms include constipation alternating with painless diarrhea, more prevalent in poorly controlled diabetes with neuropathy. Other potential causes, such as pancreatic insufficiency or medication effects, should be investigated before diagnosing diabetic enteropathy. Constipation affects up to 60% of long-standing diabetes patients, with severe cases leading to complications like megacolon. Fecal incontinence, especially nocturnal, is attributed to sphincter dysfunction due to autonomic neuropathy.
Diagnostic methods involve endoscopic examination, imaging, and other tests. Treatment focuses on symptom relief, fluid/electrolyte correction, nutrition improvement, glycemic control, and addressing underlying causes.
Liver diseases
An increased risk of developing nonalcoholic fatty liver disease (NAFLD) in people with diabetes, especially type 2 diabetes mellitus (T2DM), highlights the complex relationship between diabetes and NAFLD. NAFLD, which is known as the hepatic manifestation of metabolic syndrome, has been shown to frequently be associated with diabetes, with studies revealing a significant incidence in those with the disease.
The prognosis and clinical course of NAFLD in diabetes are impacted by the advancement of NASH (nonalcoholic steatohepatitis) and, in severe cases, cirrhosis. Notably, people with diabetes and NAFLD are more likely to develop hepatocellular carcinoma (HCC), especially if they have cirrhosis.
Obesity, insulin resistance, and metabolic syndrome are all significant variables in pathophysiology. Comprehensive management involves lifestyle modifications, glycemic control, and addressing metabolic risk factors, emphasizing the importance of regular monitoring and early intervention to prevent disease progression and associated complications.
Take-Home Points
Diabetes can affect various body systems, but particularly the digestive system. It is crucial to consult your medical team if you have uncommon gastrointestinal symptoms so you can determine the reason and explore your treatment choices.
References
FAQ on Diabetes and Digestion: How does diabetes affect your digestion?
Diabetes affects our digestion in various ways. It may lead to conditions like:
Esophageal complications
Gastroparesis
Pancreatic disorders
Diabetic enteropathy
Liver disease
Gastroparesis is a digestive condition in which food remains in the stomach for too long (delayed gastric emptying), rather than passing into the small intestine when it should.
Yes, diabetes can lead to esophageal complications, resulting in abnormal peristalsis, spontaneous contractions, and reduced lower esophageal sphincter tone. This may cause symptoms like dysphagia and heartburn.
Yes, diabetes can impact the pancreas and liver. In the pancreas, it may lead to insufficient insulin production (type 1) or insulin resistance (type 2). Diabetes is also associated with nonalcoholic fatty liver disease (NAFLD), affecting liver function.
Yes, improved glycemic control has been associated with positive outcomes in managing digestive issues related to diabetes.
Yes, maintaining a well-balanced diet, managing blood sugar levels, staying hydrated, and regular exercise can contribute to good digestive health in individuals with diabetes.
Comments ( 0 )
No Comments
Leave a Comment
Related Posts

Is Guava Fruit Good for Diabetes? Let’s Find Out!
Is Guava Good for Diabetes? Discover the benefits and effects of guava for diabetic people and know how to eat it to lower blood sugar.


Mohammad Aqdus
Benefits of black rice for diabetes, Heart health and weight loss
Know the benefits of black rice for diabetes, heart health and weight loss. Know how black rice can help lower high BP, high Sugar and weight loss in this Article.
Dr. Mrinalinee Roy
Is Beetroot Good for Diabetes Patients? Let’s Find Out!
Is Beetroot Good for Diabetic Patients? Beetroot is a superfood having many health benefits but is beetroot good for sugar patients? Read to Know.
Dr. Mrinalinee Roy

Is Banana Good for Diabetic Patients? Let’s Find Out!
Know is Banana Good for Diabetes? Discover the Health Benefits of Bananas for Diabetes. Also, know how many bananas can a diabetic eat a day.
Dr. Mrinalinee Roy
Health & Wellness Tips
Subscribe to our blog